
(As per IAP Parent Guideline Committee)
THUMB-SUCKING
My child is sucking his thumb since infancy. We thought that he would grow out of it. Now my child is 3 years old, but his habit is same. Why does my child continue to suck his thumb?
Thumb-sucking is self-soothing. It is harmless behavior of infancy and early childhood.
I have not seen such habits in other children in my family. Is it only my child who has this problem?
Thumb-sucking is not a disorder or manifestation of abnormal behavior in a 3-year-old child. Though common in children below the age of 4 years, it
does not run in families.

I have seen many parents giving pacifiers to their babies to avoid thumb-sucking. Should I try to introduce pacifier to get rid of thumb sucking in my child?
I will not advise that. Pacifiers may increase the risk of ear infections by adding germs to your baby’s mouth. Prolonged use of pacifiers may also lead to dental deformities.
Apart from doing it for self soothing, could there be other reasons for thumb-sucking in
children?
If it persists beyond 4 years of age, it could be habitual or due to psychological reasons. These include emotional insecurities, neglect, loneliness, oppressive or overcontrolling parents, family discord, etc. Children who have difficulty in gaining self-confidence resort to thumb-sucking. A child who wants to attract parental attention (arrival of a new baby in the family) may also
develop this habit.
Doctor, we have tried many things at home as suggested by my mother and other relatives to get rid of this problem. We have tried scolding, punishing by forcibly taking out his thumb from mouth, applying many bitter chemicals, plastering thumb, etc. But, all these attempts did not yield any success. Now you are the last hope. Please help us.
Have patience. Your child is only 3 years old.Punishing or scolding the child is not going to help. At times, it may even worsen the problem. Child may become aggressive or rebellious and may develop behavioral problems in later life. Your child fails to understand why you are doing all these noxious things to him.
Sir, many of my relatives and friends have
scared me by saying that thumb-sucking
may deform my child’s teeth and face. What
problems is he likely to face in future if he
does not leave this habit?
Thumb-sucking beyond 5 years may be associated
with sequelae (Dental malocclusion with open
bite or under bite, paronychia, and social and
psychological issues)
I am really scared after hearing the various serious complications which may happen to my child. I was taking this problem very lightly. Please tell me at what age we should intervene?
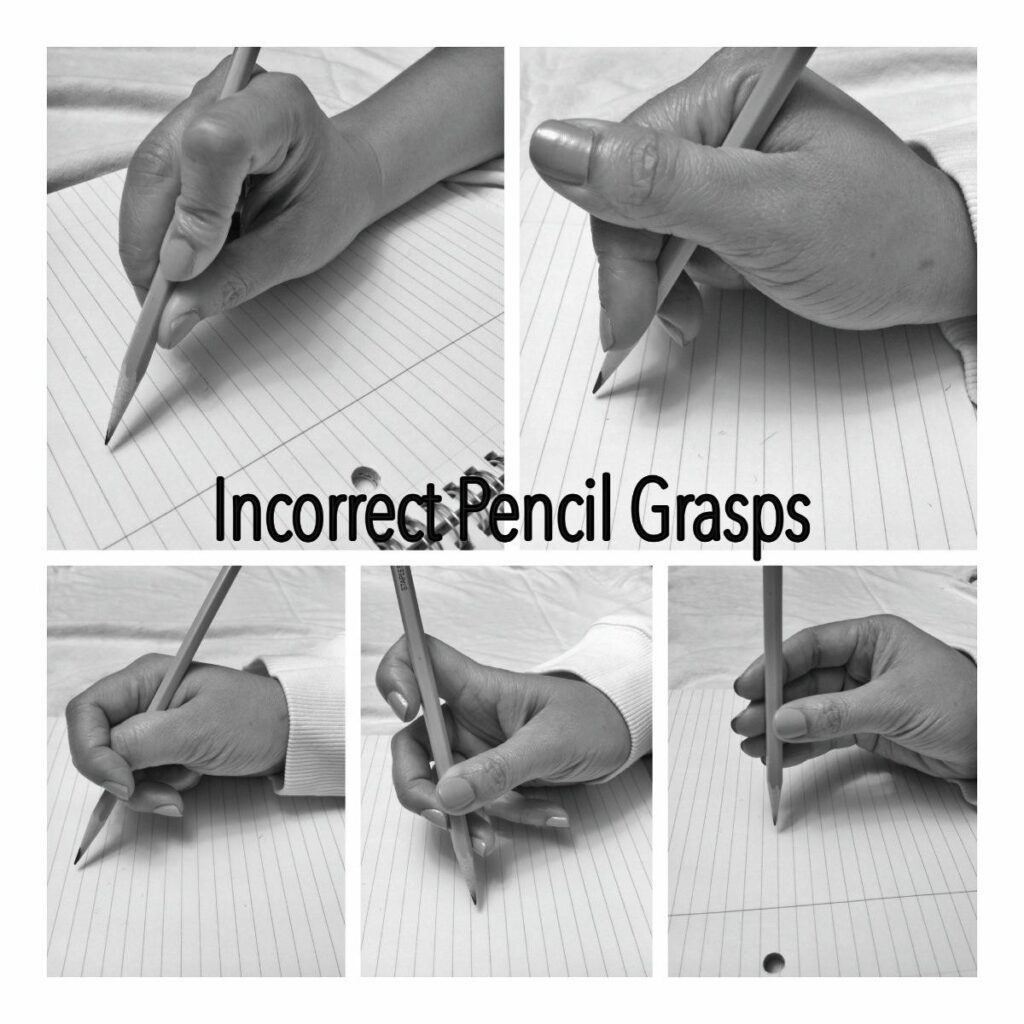
Most of the children give up this habit by the age of 4 years. If a child persists in thumb-sucking beyond the age of 4 years, we need to intervene. Developmentally, beyond the age of 4 years, you may reason with the child and obtain his cooperation in working on giving up a bad habit. You may plan on variousactivities and games which involvethe use of hands such as drawing,craft, painting, etc.
What else can we do for the bigger children who continue to do thumb-sucking?
Intervention should be preceded by 1 month moratorium on parental attention. Many a times, it is successful. If it fails, we may use following interventions:
Monitoring of the habit: Monitoring allows the parents and child to keep progress (or lag) and that provides a basis for delivery of motivational incentives. Make charts of progress and record on daily basis.
1) Motivation rewards and incentives: Praise the child for substitute behavior.
2) Sensory feedback: Application of noxious, bitter nail polish which is applied over the nails only. It can be used two-to-three times a day. Child must be told about what you are applying. Most of the children improve in 2 weeks and do not require further treatment.
If some complications occur, whom should we consult?
Dentist opinion and intervention is a must, if there are malocclusion and abnormal facial features. Orthodontic appliances for correction are needed.
Orthopedic approach in the form of thumb guard hand stopper, palatal arch, and palatal crib may be worth a trial. In resistant cases, fixed intraoral antithumb-sucking devices may be used, though very rare.

DO NOTs OF THUMB-SUCKING
- DO NOT intervene till 4 years of age.
- DO NOT use force to stop thumb-sucking like tying the limbs and slapping the hands.
- DO NOT use aversion techniques such as dipping the hands in un pleasant tasting substances as it may lead to frustration and rarely poisoning.
- DO NOT delay the treatment, if there is dental malocclusion or abnormal facial growth.
TEMPER TANTRUM
My 2-year-old daughter does not listen to us at all. Whenever her demand is not met, she starts crying and kicking around. What is it?
Your daughter is showing temper tantrums. Temper tantrums are one step higher than just anger or demanding behavior. A temper tantrum is a behavioral episode
characterized by extreme anger and frustration. The child will express her frustration by excessive crying, screaming, and violent body motions such as throwing things,
falling to the floor, or banging her limbs or head against the floor.
If we fulfill her demand every time, will it help in avoiding these episodes?
As a parent, you may think that giving in to the child’s tantrum is a
tempting option. However, this could be counterproductive. It might reinforce in her the notion that she could get everything she wanted by simply throwing a tantrum. It is equally important to follow reasonable rules and maintain disciplined behavior. She has to obey these rules with willingness. It is only possible once you discuss the problem when she is cool, calm, and ready to understand what is said by you.
Can you do something to reduce the duration of the tantrum episode?
A temper tantrum is an attention-seeking behavior. One way in which
you may minimize the length and severity of the tantrum is to ignore
the child’s behavior when she throws a tantrum. Provided that the
child is safe and is not behaving in
a destructive manner, keeping her
alone in a room may work because
there would be no one to react to
the behavior. Sometimes, she may
still persist with her tantrum. In
such a case, do not talk or react to
the behavior until it stops. Once the
episode stops, calmly discuss the
issue, justify your behavior, and offer
the right alternatives.
I have seen the children of my friends in the same age group. They do not have such a problem. Why does my child have this problem? Are we not parenting her well?
Please do not doubt your parenting. Temper tantrums (also called “acting-out”) are natural behavior during early childhood. As children grow and develop, they begin to
view themselves as distinct entities that are separate from their parents. As a result of this, they begin to try to assert some independence. Occasionally, children may throw
a tantrum in order to gain attention from parents or caregivers or to manipulate the situation to suit their wants. Tantrums are also worsened as a result of a child’s limited vocabulary which impedes their ability to express themselves effectively. Certain conditions such as being exhausted, hungry, or sick may worsen a tantrum or increase
their frequency. Rest assured that it is not at all a sign of bad parenting.
How to manage the child during a tantrum episode?
It is important to remember to keep your cool and stay calm when responding to a tantrum. It is not the right time to try and convince
logically or make the child understand when she is throwing a temper tantrum. It helps to remember that tantrums are normal. Reacting by shouting and/or hitting the child will only worsen the situation. When responding, do
not bend the rules that you have set or give in to the child’s unreasonable demands. Maintain a quiet and peaceful atmosphere in
order to contain the amount of stress that you face. Try to create an environment in which both you and your child feel better suited to
bringing the tantrum to a resolution. When the child throws a tantrum away from home, lead the child to a quiet place like the car or a toilet. Ensure the child’s safety until the
tantrum has subsided.
Can you do something when a child is about to show a temper tantrum?
Are there any tell-tale signs which indicate that your child is going to have a tantrum episode?
Yes, it may be possible to mitigate an episode by being alert to certain danger signs, especially fatigue, hunger, and irritability. You may have to change your immediate plans and give the child the needed food, rest, or change of place and
scene. Gentle distraction by engaging the child in playful activities that amuse her may also work.

How can we prevent tantrums?
The acronym C.A.L.M may help with remembering how to prevent a temper tantrum.
1) Communicate well: Children pick up a lot through the means of social learning. Parents must set a precedent for the children to emulate by modeling excellent
communication skills and must avoid getting into arguments or raising their voices in front of their children. Toddlers may benefit from being presented with facial depictions of feelings (such as a tragic face, angry face, and happy face) and allowing them to pick the image that best describes their feelings. It is also essential to teach older children to use their words to express their emotions.
2) Attend to the child’s needs: Make sure that you are providing positive attention to the child such as reading to her, playing games with her, and including her in routine activities such as cooking and cleaning. It may also be useful to offer her age-appropriate toys in order to take her mind off of exploring unsafe or undesirable objects. Maintain age appropriate expectations of your child’s behavior. Limiting her exposure to violent television viewing will also help.
3) Let the child share her feelings: Try to minimize the use of the word “no”. In an event that does not pertain to a health or safety issue, it may be alright to let the child make a choice that may not align with your preferred alternatives, such as wearing mismatched clothing.
4) Make nap-times and meal-times a part of regular schedules with some latitude: In case, the toddler is away from home or misses her scheduled meal-times, keep simple and healthy snacks such as fruits or crackers at hand.
Till what age will my child continue to show temper tantrums? Is it likely that these will hamper my child’s development?
The onset of temper tantrum usually occurs between 12 and 18 months of age. In due course of time, children learn to identify feelings, name their emotions, and utilize positive means of coping with negative emotions as they grow older. Temper tantrums become infrequent after the age of 4 years. Generally, typical temper tantrums in toddlers have an excellent prognosis. They are a part of normal childhood development and the child usually stops them by the time he reaches school-going age. There are no long-term side effects on development or behavior.
What to do if a tantrum starts in a public place?
Children become overstimulated or tire more easily in busy public spaces such as malls, public functions, etc. In such situations, they use the tantrum as an effort to regain parental attention when they are busy somewhere else. Despite their understandable embarrassment, parents ought to treat a public tantrum in essentially same way as they treat one at home. Whenever possible, they ought to remove the kid to the car or another private space to avoid inconvenience to others and attracting any unwelcome attention.

Are there any medications that help?
It is important to keep in mind that temper tantrums are benign. Prevention is the best antidote to frequent and recurrent temper tantrums. Paying attention to common triggers such as fatigue, hunger, illness, or injury may help. In rare cases, medication may help in management of associated extreme behavior such as breath-holding or aggression. Iron therapy has been found to be helpful in reducing the frequency and severity of breath-holding events in children
with iron deficiency. In case of injury, it may be necessary to provide necessary medical attention. Medication without consultation with your doctor may be harmful.
PICA
My 8-month-old son puts his toys into his mouth. I am worried. Will this become a habit for him in future?
This is no cause for concern, as all toddlers have this habit, which is often called mouthing. This is regular
and standard phenomenon and is normal instinct of toddlers (like many nonhuman primates) so as to assess
the edibility of any substance they encounter while playing around. If thishabit continues beyond 2 years of age,
we may suspect an eating disorder known as “pica”, and then a medical consultation may be warranted.
What is “Pica”?
“Pica” is basically an eating disorder. Usually, a person eats only standard edible items such as fruits, bread, milk, etc. In “Pica”, the child eats nonedible items such as wool, clay, soap, paint, earth, ashes, etc. If this feature has lasted for over a month, then medically it is termed as “Pica”.
Does pica occur only in children?
No. It can occur throughout lifetime. But it occurs most commonly in child hood.
Which children are more likely to have this eating disorder?
Children with malnutrition, specific nutritional deficiencies (e.g. calcium, zinc, and iron), and children who are facing neglect or are in poor family environment are more likely to be affected. It is likely to be more common in children with intellectual disability, autism, and schizophrenia. Therefore, a proper assessment of the child is important.
How can I confirm that my child suffers from pica?
There is no confirmatory test such as a blood test or X-ray, etc. The diagnosis is made on certain criteria. These include:
1) The child must have been eating these non-nutritive non-food items for over a month.
2)The eating must be abnormal for the child’s age and level of development (it may be a normal situation for an infant or toddler to mouth items that come to its grasp). A minimum age of 2 years is mentioned for the same reason.
3)The eating should not be associated with any culturally accepted practice, which is considered normal in the social context of the child (just as a pregnant lady may have peculiar taste cravings).

My colleague’s 13-year-old daughter scrapes off paint from the walls and chews that. What should they do?
This will require a good evaluation of the child. Deficiencies of iron, vitamin D, calcium, and zinc need to be excluded, or even a trial of these medications may be given. Behavioral and psychological assessment will have to be done, and relevant intervention and counseling may be required. In most situations, counseling does help.
My cousin lives in Ghana, and she says mud-eating is a common practice there particularly in pregnant women.
This is called “Geophagia”. This is actually associated with pregnancy and is considered normal for them. This is accepted in some rural communities in Africa as a normal cultural practice.
How long is this habit likely to continue?
Pica mostly disappears by teenage. At
times, it may persist into adolescence
too.
Are there any medicines or specific treatment for this condition?
Any deficiency disorders, particularly iron deficiency must be treated and any mental issues evaluated and treated likewise. Any family issues such as parental discordance, etc. should also be addressed.
What can I, as a mother, do to help my child get rid of this habit?
Apart from following your pediatrician’s advice, please give your child good nutritious food from your regular family bowl. Avoid any negative impacts on the child’s brain and psyche (parents quarreling, other members of the family shouting at each other, bad mouthing others in their absence). The family environment needs to be conducive to proper mental development of the child.
Is there any possibility of any serious issues developing out of this habit, if it cannot be prevented or controlled?
Usually “pica” in itself does not create any serious problems. However, children with pica are at increased risk of lead poisoning (caused by paint eating), worm infestations (mud or feces eating), iron deficiency anemia, etc. All these will have to be treated appropriately. Some children have the habit of tearing their own hair and eating these. These bits of hair may entangle and get stuck somewhere in the stomach or lower down in the alimentary canal. This may require treatment including surgery to remove the ball of hairs (Trichobezoar).