

Feeding Children with Special Needs

……..developing the first ability to meet one’s needs
Babies have an innate ability to feed; this is well demonstrated in their ability to-
- turn their head to seek the breast when their cheeks are stimulated (rooting )
- suck and swallow (reflexes) when breast is introduced into mouth
- cry when hungry
These skills gradually increase with time and become more mature, they acquire additional abilities which enable the baby to eat out a variety as they approach their first birthday. They first learn to use their lips and tongue to suck and swallow liquids. Later they learn to chew and bite solids and finally to take their food with their hands. At this time a keen mother finds that her baby’s head-turning and sucking reflex are no longer present. But all is not that easy, even for normal children and mothers, not to mention those children who have any physical problems or brain damage / slow development. Thus feeding initiation and continuation may be especially difficult for such special children, say with cerebral palsy, because they may have difficulty with sucking/swallowing. Many times such difficulties/ even absence of suck may be an early pointer to the catastrophe which is yet to manifest!! Sometimes sucking may be there, but they get choked quite frequently. This is usually due to uncontrolled/ trouble in swallowing, uncontrolled body movements, inactive baby (floppy) / inactive lips- all may contribute to feeding problems.
Another reason for babies not developing such skills is either an overprotective parent/ indifferent parent. They may be slow because their parents continue to do everything for them; they continue to treat them as a baby! Rather than encouraging them to try to feed themselves, parents may continue to feed.
Feeding facts- Special Needs Children
- Help the child develop feeding skills as early as possible.
- The food needs of a special child are the same as for any child.
- Special children are often in greater danger of malnutrition than are other children.
- It is important that disabled children get enough to eat.
- It is important that they do not eat too much and get fat.
- Extra weight makes it more difficult for a weak child to move about.
- If the child is getting fat, give them less fatty foods and sweets.

The best food for my child?
FIRST 6 MONTHS
Breast feeding …..???, YES, only breast feeding!!
Breast milk is the best milk. It is clean with ideal contents to suit your baby, at the right temperature, and readily available. There is no need to boil and it contains all protective antibodies for your special child. Many such special needs children, for eg: Down’s syndrome may have frequent infections, hence breast milk is ideal for them.
- “I have milk but baby doesn’t suck/swallow!!- don’t teach me theory doctor………be practical”.
If baby cannot suck, you can express milk and feed her with cup and spoon. Please do not use bottle. They are often storehouse of infection.
- How do I express my milk?
Manually with your hand/ with a breast pump- manual, semi-electric / electrical. But use a good quality pump; no point in wasting money twice / thrice by buying cheap alternatives. Buy one good only once! May be Aventis/ Madela.

6 MONTHS- 1 YEAR
Continue breast feeding; also start the baby on other foods-juices and fruits, mash of green leafy vegetables, beans (boiled, skinned, and mashed), peanuts (skinned and mashed), egg yolks, and other local staples such as rice, corn, plantains etc.
Small stomach’s need food often. Feed children under 1 year old atleast % times a day – Give snacks between meals.
If the child has trouble in eating solid foods, do not keep giving only milk or formula or ‘rice water’. Mash or grind up other foods to form a drink or mush.
By 8 months to 1 year of age the child should be eating the same food as the rest of the family – even if it has to be mashed or turned into liquids. But in special children, the more difficult it is for child to control their body movements, the more difficult it will be for them to feed themselves.
Feeding problems includes
- Lack of control of mouth/head/body
- Poor sitting balance
- Difficulty in bending hips to reach forward
- Poor hand – eye coordination and difficulty in holding things and talking them to mouth.
- Poor sitting balance
We must consider all these things when trying to help the child feed more effectively. It is not enough to simply put food or pour drink into the mouth of a child who has difficulty sucking, eating, and drinking. We should find ways to help the child learn to suck, swallow, eat, and drink more normally and effectively.
How do we feed them?
Positions for feeding
Ensure that you keep your child in a good feeding position BEFORE you start feeding them. The position you keep makes feeding either easier and safer, or more difficult and unsafe for the baby.
- Never feed child while they are on their back as you increase the chance of chocking by doing so.In a child with cerebral palsy, it often causes backward stiffening, and makes sucking and swallowing more difficult.
- Never make the head tilt backward. It makes swallowing harder and increase the choking hazard.In a child with cerebral palsy, avoid pushing the head forward by supporting the occiput (prominence at back of head). It will cause the baby to push their head back more forcefully.
- Feed the baby in a half sitting position with their head bent slightly forward.

- In a child with cerebral palsy, to keep the head from pushing back, hold the shoulders forward, keep the hips bent, and push firmly on the chest. Positions for feeding with a spoon or finger are like those for breast feeding.
- To avoid the backward stiffening, bend the shoulders and back forward, keeping the hips and knees bent. Be sure the head bends a little forward.
- Place food below and in front of child, not above or behind him. A simple ‘baby seat’ can help the baby hold a good position while eating.
- If the child is pushing too much backward/ a big child, allow the child’s bottom to rest on floor with hip and knee flexed. Keep one leg of yours over both feet to keep them flat. Keep the back straight and neck slight flexed forward and start feeding.
Controlling jaw functions
Most of these children will need help in improving the sucking-swallowing reflex, and their ability to eat with a hand or spoon and to drink using a cup. We can be improve this by using what is called ‘jaw control’.
“Jaw control” is given by two ways-
- Sitting beside the child- keep your thump over jaw joint, index finger under lower lip, middle finger under chin(be sure not to press-in the soft tissue under chin)
- Sit facing the child -index finger over jaw joint, thump between lower lip and chin, middle finger pressing chin from under.
At the start, the child may push against our hand, but once the child gets used to it, it will enable them to get control of movement of mouth and tongue. Ensure that you do not push their head back, but keep it bent forward slightly.
Apply gentle and firm, steady pressure with fingers, Not On and off.
Along with a good position and jaw control several problems common in cerebral palsy, such as pushing the tongue forward, choking, and drooling (dribbling) can be reduced. As oral control improves, gradually lessen and finally stop jaw control. After trying for 2-3 weeks , if the child still resists /shows increased problems, better stop jaw control.
Spoon feeding
The child who has no sucking-swallowing reflex needs to be fed with a spoon. Always give the spoon from front, not from side or behind or from above while lying supine!! Spoon has to be placed flat on tongue with firm down ward pressure. See if baby is closing mouth slowly; if not help them to close the lips. Keeping the spoon flat, quickly, but gently remove the spoon. Ensure you are not pulling it against the upper row of teeth. Keep mouth closed and maintain the pressure so that baby starts using the tongue.
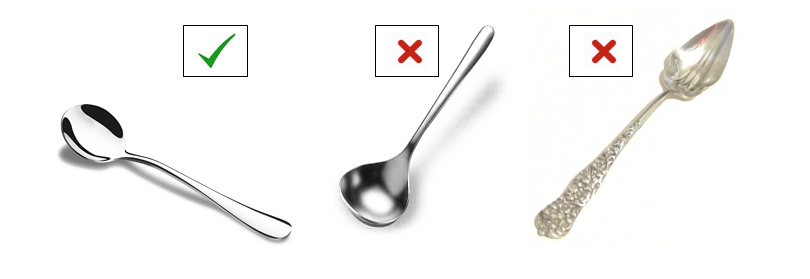
The best spoon you can select is a shallow and rounded one- NOT a deep one as it is difficult for child to swipe food out of it. A long and pointed spoon is better avoided as it induces choking. No plastic spoons as they may break.
Tongue thrusting
One of the commonest problems encountered during feeding a CP child is tongue thrust. During sucking at the breast, they move the tongue forward and backward. Hence as they take food at the starting, they do the same resulting in tongue thrusting. But, soon babies learn to use their tongue to bring food to under their gums, to swallow. This is delayed in many special children. Don’t be of the impression that they do it as they hate the food.
What next? First do the jaw control. Then, apply firm pressure with the back of the spoon on the tongue as you feed the child. This keeps the tongue inside and prevents from pushing forward and lets the child use their lips and tongue better. Better to use a metal spoon as plastic ones may break.
It is a common practice to scrape the food onto the upper teeth or upper lip as we take the spoon out. Never do it on a special needs child. Instead, let the child try to get the food off the spoon onto their tongue. To make it easier for them, start by putting only a little food on the end of the spoon. As you take the spoon out, make sure the mouth is closed so that the tongue can move the food inside the mouth and cannot push it out. If eating with fingers is the custom, or if spoon-feeding is too difficult, use your fingers. It is best to start off with soft, mushy foods rather than liquids. Milk (even breast milk) or egg yolk can be mixed with rice paste, boiled corn, or mashed beans. South Indians typically start with Ragi with jiggery paste also. You can also give small pieces of fruit, mashed greens and vegetables, and yogurt or soft cheese. Hardest for the child to eat are combinations of liquids and solids-such as vegetable soup.
Chewing
You can make them learn to chew by putting a bit of firm food in the side of her mouth between their teeth. Use very small pieces of bread crust or chapatti. Help to close their mouth using jaw control. Biting off can be encouraged by pulling slightly on a long thin piece of food or by rubbing a piece of food against the teeth before putting it between them.
Never open and close the child’s jaw or help them chew. After they bite the food, their jaw must stay closed or almost closed to chew. To help in this, we can apply steady firm pressure with jaw control. This makes the child to make chewing movements. Make the jaw move on its own, but do NOT make chewing motions for the child! This will only encourage abnormal movements.
Drinking
Body position is important for drinking. For a child with CP, to drink from a regular cup or glass, his head must be tilted back causing uncontrolled backward stiffening and choking.
However, if we use a plastic cup with a piece cut out, drinking can be facilitated without bending head back. At first we need to apply jaw control to help the child close lips on the rim of the cup. Tilt the cup so that the liquid touches the upper lip and let the child do the rest. NECER take away the cup after each swallow since it triggers pushing the head back or tongue out. Start with thick liquids-like cooked cereals, maize mush, or yogurt.
Self-feeding
Feeding self requires the child to control of the mouth, lips, and tongue; able to sit with head up; to pick things up, and to bring to their mouth.
Preparation for training self feeding can be started first by encouraging them to bring toys or hands to their mouth first. Increase their sitting balance by encouraging them to bring hands forward off the ground while sitting. As the child brings the hands to mouth ot things to mouth, we can train on use of hands to self feed.
Start with a food the child likes and if possible colourful. Make the child manipulate the food. Then lift the fingers to the child’s mouth. Help child to do more and more, step by step, until child does it alone. Slowly just lift tha hands alone towards the lips and see if they open mouth and put it in mouth. The fade off the help by just lifting the hand near the mouth and see if child will do the rest. Next just put finger in the food and encourage child to take it to its mouth. Give generous praise and motivation each time the child attempts and succeeds.
Oral defensive activities: what to do?

- A NUK oral massager for the gums (found in most pharmacies) we use this across his gum, tongue and around the sides of his mouth.
- A small finger brush (a little thing that fits over the finger and is used to brush the baby’s gums
- Food of all textures and temperature
- Lot of positive reinforcement during eating
2 Comments
Leave a Reply
Hi Test
Yes Test